Decreasing Heart Attack Risk: Does Losing Weight Help?
May 24, 2024
[TLDR: A ten-year-old study shows that losing weight does not improve heart related outcomes in a patient population that suffers from Type 2 Diabetes and obesity. Is it possible that the reason they failed was the method they chose to help people lose weight (calorie counting)? Hat tip to Gary Taubes for mentioning this study somewhere and prompting me to go looking for it.]
Imagine that you are at high risk of cardiovascular disease - a heart attack or a stroke. You know this because you suffer from type 2 diabetes (T2D) as well as obesity (you're overweight). People with T2D are very likely to suffer a premature heart attack. In a large percentage of those cases, the first heart attack is fatal. What can you do to lower your risk?
You might think that one thing to do would be to lose weight. And if you want to lose weight, most "experts" will tell you to eat less and move more. So would losing weight in that way be a good thing?
Fortunately there was a study that looked at exactly this question about 20 years ago. Most of the nutritional research that’s out there suffers from some serious problems. It relies on food frequency questionnaires or observational data to try and make conclusions about diet and nutrition. So for example we know that people in Hong Kong are very long lived. Is that because people in Hong Kong eat the most dim sum? Is it because they eat the most meat? Or is it for some other reason - proximity to the sea or being a semi-autonomous city state or something else? There’s no way to know what’s causing the longevity without doing some actual real-world tests.
The Look AHEAD trial attempted to do those real-world tests. Unlike the vast majority of nutrition research out there it was an actual Randomised Controlled Trial (RCT). That means taking two groups of people, giving one an intervention and one a control (no intervention) and seeing how they do over time.
Would it be ethical to take a group of very high risk patients (all of these people had T2D and many were obese) and give half of them a lifestyle intervention that was thought to be beneficial and half of them nothing? Maybe not.
The research team got around this concern by providing some support to the intervention group. So they got what the research team called “diabetes support and education”. They had access to some support at least and they were given recommendations that were similar to those given to the intervention group (but not monitored).
What did the intervention arm get exactly? For the first six months they had to check in with a medical and nutrition team weekly. After that period the frequency reduced to every other week for the next six months or so. In years 2-4 there was one in-person session and at least one session by phone per month. After year 4 they had monthly in-person sessions as needed (at least once per month).
What was the medical advice? Severe caloric restriction. For those who were less than 114kg (250 lbs) the calorie goal was between 1200-1500 calories per day. For those heavier than that, the goal was 1500-1800 calories per day. ("Calories" is not the right term, as I've written about here, but we know what they mean.) As someone who’s done a lot of research on these topics, my guess is that that’s less than half of what those people would normally have been eating. So this was a dramatic intervention. The intervention was justified, in the eyes of the researchers at least, because these people were in a very high risk group. They were also encouraged to do a bit more physical activity than the placebo group (175 minutes per week as opposed to 150 minutes per week in the placebo group), though the study doesn't provide data on whether the participants followed the new exercise routine, though they did receive some coaching in the early phase.
In terms of the makeup of the diet, the supplemental materials reveal that the macronutrient ratio was 30% fat and 15% protein. Basic math tells us that the remaining 55% was carbohydrate. So this was neither a low fat nor a low carb approach and it's very close to the macronutrient ratios in the Standard American Diet (SAD). The acronym is a good descriptor.
In terms of the research, this is a good thing. Not good for the participants (there was already data that this macronutrient would be disastrous for those poor participants, as Denise Minger has documented). But it is good in terms of the scientific method. Those ratios are probably very close to what the participants were already eating. So it isolates a single variable - calorie restriction, or maybe two variables with the exercise component as well.
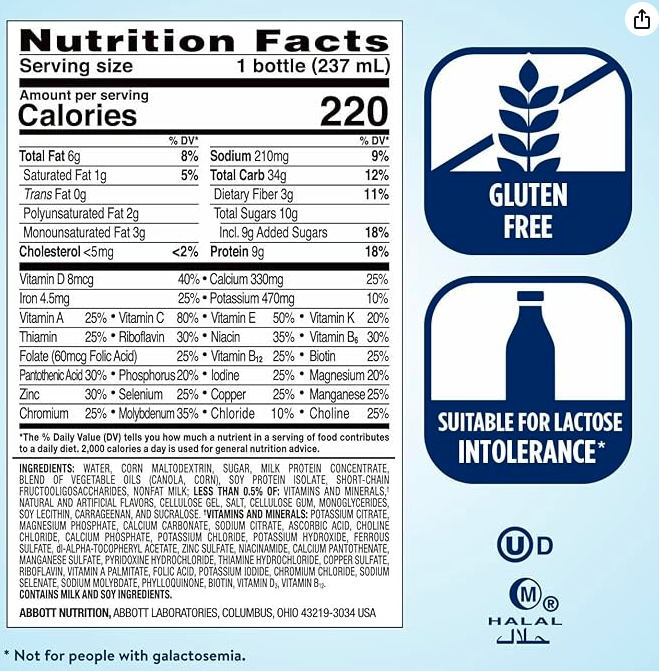
In order to hit the calorie targets, participants were encouraged to replace meals with shakes and snacks with a snack bar. The ingredients on these are not given, but it isn't hard to guess what was in those processed "health" foods - seed oils, sugar and other sweetners, maybe high fructose corn syrup. If you doubt the inference I'm making, just consider the kind of meal replacements that are (still!) recommended to cancer patients, like Ensure. Here's the nutrition information for Ensure:
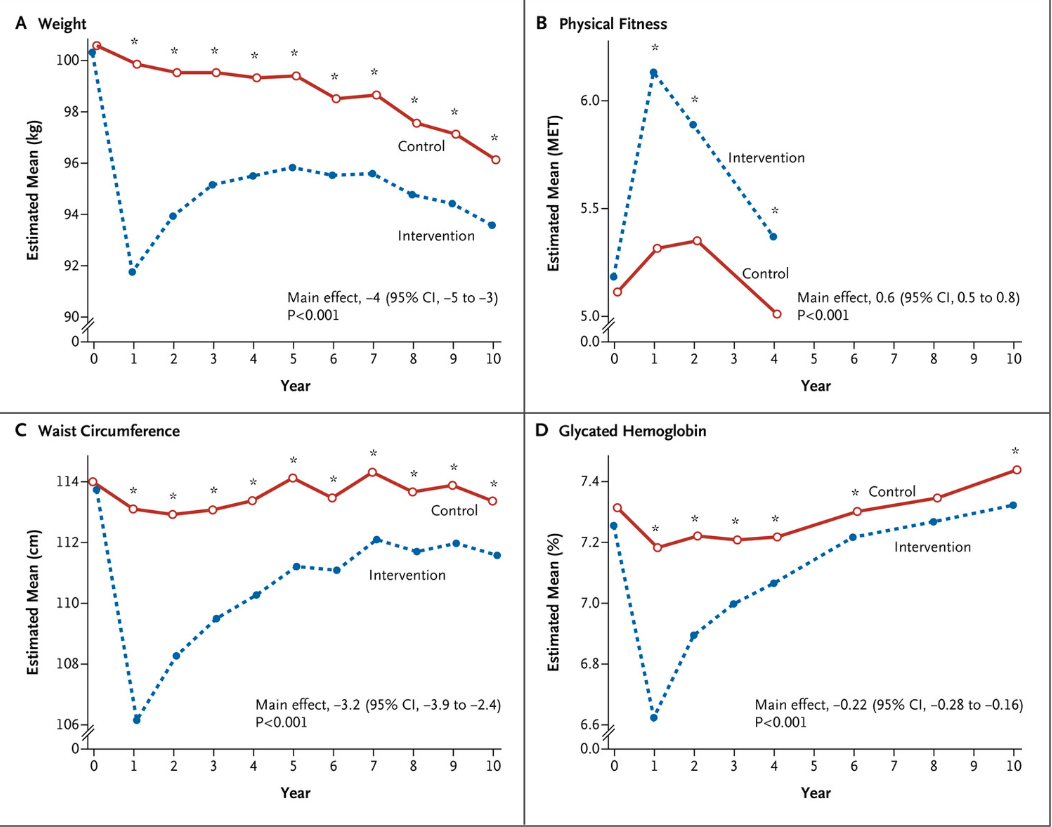
So after all this advice, all this follow up, and all this counselling, what was the end result? The people in the intervention group were indeed able to reduce weight; it was pretty significant in the first year and then became less and less as their basal metabolic rate tanked from the calorie restriction. This pattern held for A1C, waist circumference and physical fitness as well.
They did well in the first year and then less well year after year thereafter. But that weight loss did not translate to a significant reduction in events like heart attacks or strokes or in all cause mortality. In other words the people who were just going about their lives as they normally would died of heart disease at pretty much the same rate as those who were torturing themselves in an effort to lose weight. This chart is pretty telling. The two lines are almost indistinguishable.
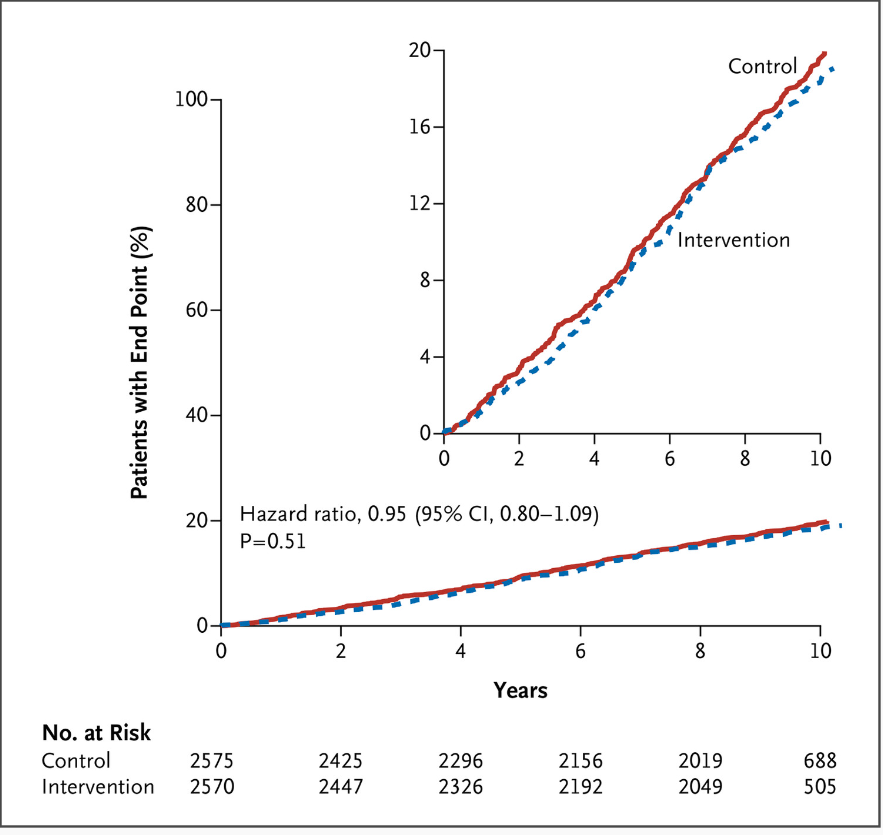
In terms of RCTs, that's pretty much rock bottom there. The two arms of the trial - the control and the intervention group - are almost indistinguishable when it comes the primary endpoints - heart attack, stroke, death or hospitalisation due to heart disease. The number of people suffering from any one of those did not differ significantly between the two groups.
Before we go deeper, let's zoom and enhance on the chart showing weight loss.
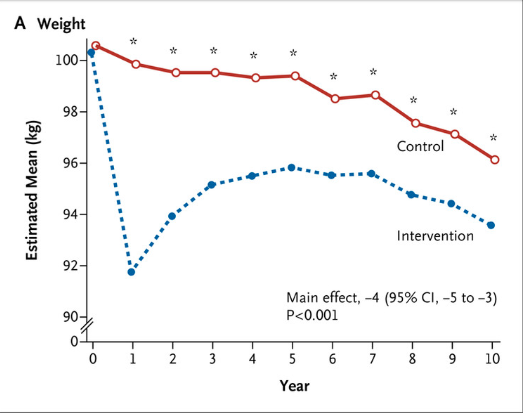
That dotted line is fascinating to me. Why? Because it looks almost identical to what we see in every study that looks at caloric restriction. Consider the data from the Biggest Loser study. This was a much smaller group of people, but we see the same pattern. Because it was a small data set we can actually give every individual their own line - this graphic was done by the New York Times.
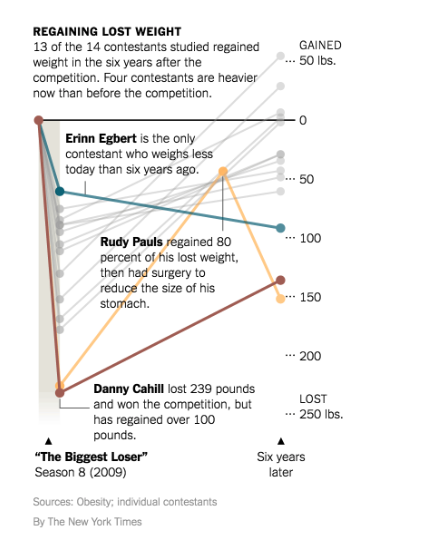
So this is a pattern that we see across studies done on calorie restriction. People on calorie restriction lose weight in the beginning, sometimes a lot of weight and then they put it back on. In the case of the Look AHEAD trial, they put it back on even though they were still eating the same amount as they were in year one. Why would this be the case? They were eating at a severe calorie deficit so one would expect that they should have continued to lose weight.
The answer is pretty obvious. Remember that these diets are so severely calorie restricted that they’re actually alarming. Going from 3,000 calories per day to about 1,500 calories per day is a shock to the system. And the system has to respond. It responds by adjusting the BMR - basal metabolic rate. The BMR is a measure of the energy your body expends to keep you alive when you're not doing anything else - keeps your heart beating, your brain functioning, your lungs breathing and importantly to keep you at a certain temperature.
We know from other data sets that when you calorically restrict your body does lots of things to lower your BMR. You may be eating less, but now your body is also going to expend less. One of the things your body does when you restrict calories is lower your temperature. That's a significant change, but it's probably not the only one. Women who go on calorie restricted diets can lose their cycle. Because the BMR goes down - it has to go down - with this kind of severe calorie restriction, the results even for weight loss are not great. You lose the weight in the beginning and then you gain it back as the body adapts. Even worse, if you ever stop calorie restriction, you're going to gain that weight back because now the body is expending less energy at rest making it easier to put on weight.
And the results for the primary end points related to heart attacks, strokes and so on were to bad that the study had to be stopped years before it was scheduled to be stopped because they could already see that the intervention wasn’t working.
Now when a study of this kind has to be stopped early that’s a disaster. It means that the the treatment arm was so ineffective, they didn’t even need to complete the trial. And because of the disastrous end to this trial, most people (and especially most cardiologists) believe that the takeaway is that weight loss is always ineffective for improving outcomes.
But that's not what this study shows.
Why doesn't this study prove that losing weight never helps cardiovascular disease outcomes? Because there are many ways to lose weight. The specific way that this study used to get the participants to lose weight is, in my mind at least, the most difficult and least effective way to do it. Does the study prove that calorie restriction isn't great for improving heart outcomes? Yes.
What about other weight loss strategies? There are other studies, not as big or as well funded as this one but studies nonetheless, that indicate that ketogenic diets - so that’s high-fat, low-carb diets - lead not only to weight loss but also to improved outcomes for cardiovascular disease. This paper from 2023 goes over some of the data we have on why ketogenic diets tend to improve outcomes. The graphical abstract does a pretty good job of summarising:
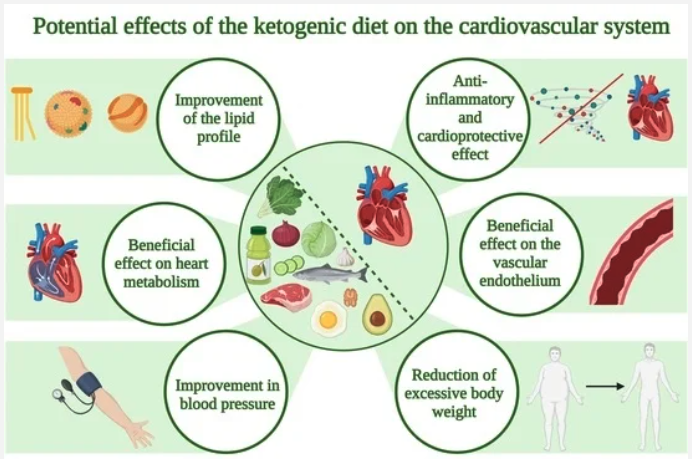
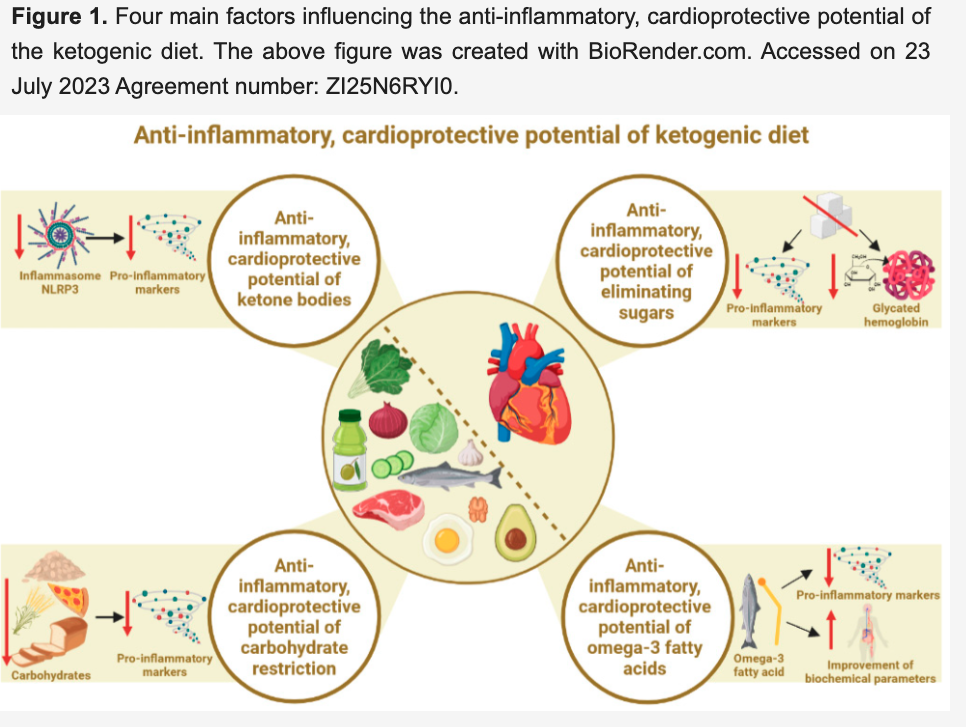
Let’s just take a look at one of these mechanisms, the inflammatory mechanism. Low carb ketogenic diets actually do two things that are known to reverse inflammation through two different pathways. When our bodies enter a state of very low blood sugar, ketone bodies are produced from fat. Those ketone bodies are increasingly being thought of as the better fuel for brain and the heart. And there are benefits to reducing the intake of sugar. This diagram gives a pretty good overview.
There is a lot of data to show that using ketogenic diets to lose weight instead of calorie restriction to lose weight does have a profound effect on heart disease. (If you doubt that have a look at the footnotes in the above paper.) But do we have Randomised Controlled Trials (RCTs) to back that up? Unfortunately not.
The Look AHEAD trial teaches us what not to do. If you lose weight through calorie restriction in an effort to reduce your risk of cardiovascular disease, you will almost definitely fail to do so. You'll probably fail to lose weight; if you do lose weight you'll probably regain it, and even if you keep the weight off you won't improve your risk of getting a heart attack. But if you adopt a low-carb, evolutionary appropriate ketogenic lifestyle you probably will improve your chances of living a long and healthy life free of cardiovascular disease.
If there’s one takeaway here it’s that no one should be counting calories. It is a really bad strategy for everything health related. The one demographic that swears by it are the bodybuilders who indeed do see success with this tactic for their particular goals - which are around body composition. But when we look at the health related data, we see that bodybuilders may be prematurely dying at higher rates than the general population - hardly a point in favour of calorie counting.
My starting point with any recommendation is the Hippocratic oath - first, do no harm. In the case of calorie restriction, the harms seem to be well documented. So whatever your health goals might be, think long and hard before you use calorie restriction as a strategy to achieve those goals.
🌱 Ready to Find Your Path to Gut Freedom?
Stop trying to solve your Crohn's, Colitis, or IBD alone with conflicting advice. A personalized plan is the fastest way to clarity and relief.
On a free call, you’ll get:
✅ Clarity on your triggers – Identify the dietary and lifestyle factors uniquely impacting you.
✅ A tailored starting point – Get actionable steps to reduce inflammation and calm your gut.
✅ Real answers – Ask anything about your symptoms and healing (no topic is off-limits).
💬 “Working with Sameer gave me a clear path when I felt completely lost. This is the guidance I needed.” – Previous Client
Your personalized plan is a conversation away.
