Plaque Begets Plaque, ApoB Does Not: The Study That Turns Heart Disease Theory Upside Down
Apr 14, 2025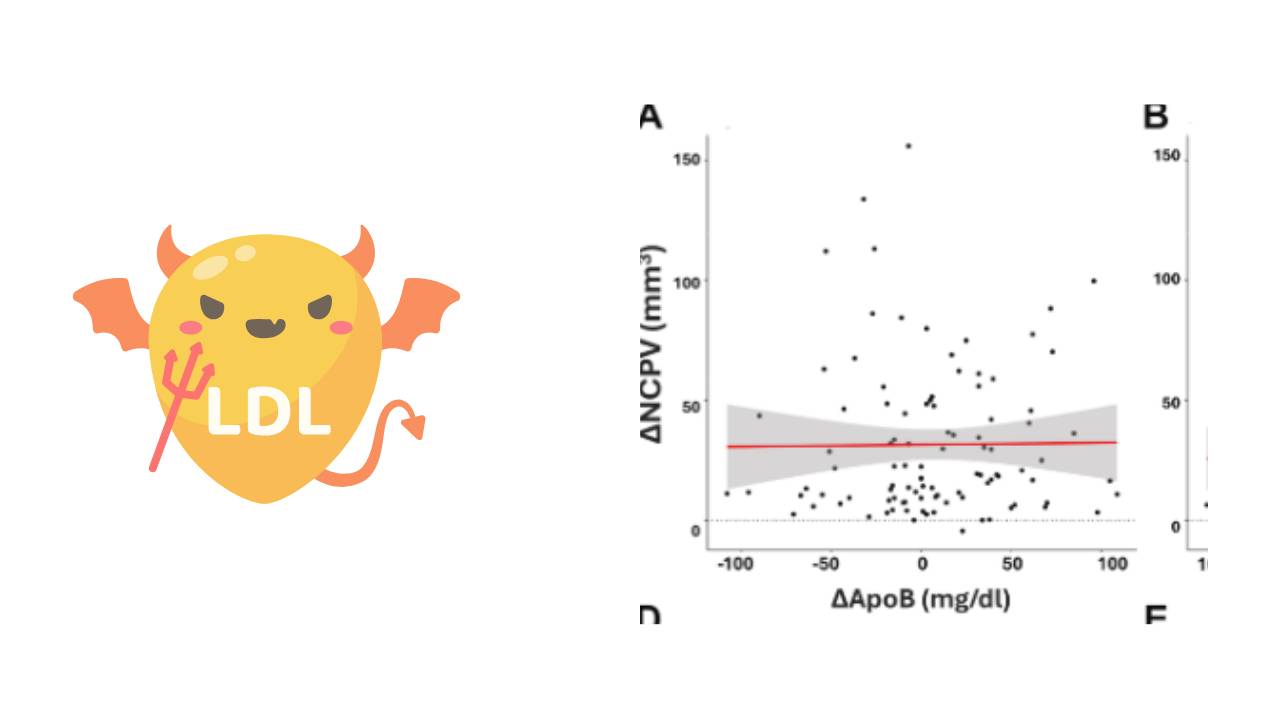
[TLDR: A new study (Plaque Begets Plaque, ApoB Does Not) disproves the long-held hypothesis that high ApoB (e.g., LDL) directly causes plaque growth in arteries. Despite participants having elevated ApoB for years, plaque progression correlated only with existing plaque—not LDL levels. Critics miss the point: science isn’t about proving LDL is harmless, but about disproving the idea that it’s always harmful. The real question now: If not ApoB, what actually drives heart disease? For those interested in my perspective, do check out the free training here.]
Science is a strange animal. In popular culture we tend to think of science as a kind of religion. Beginning a sentence with the phrase “science tells us that” is a sure way to get the person with whom you’re having a conversation to take whatever comes next seriously.
And occasionally the scientific method, with it’s emphasis on replicability, has come to conclusions that turn our understanding of the world on its head. The idea that the earth revolves around the sun is one such celebrated revelation.
But these big changes are few and far between.
In practical terms the best we can hope for in science is to be able to formulate a hypothesis that seems plausible and then design experiments that seek to disprove that hypothesis. A genuine attempt to disprove the hypothesis is crucial to the scientific method. To give one example, based on my experience growing up in Washington, DC I could formulate the hypothesis “all birds fly”. And if I only had the example of birds native to the USA, I would believe that the hypothesis is true. After all, pigeons fly, seagulls fly, bluebirds fly, etc. But none of those (correct) observations conclusively prove the hypothesis. It only takes one trip to Australia and one sighting of one emu to disprove the hypothesis. If there’s a single species of bird that doesn’t fly, I have to go back to the drawing board.
And it is in this context that we must understand the recent release of a study entitled Plaque Begets Plaque, ApoB Does Not: Longitudinal Data From the KETO-CTA Trial. The study is the first in what promises to be an intriguing set of studies released by Dave Feldman and his team, including Dr. Matthew Buddoff at the Lundquist Institute.
In the week since the data has been released, there have been all sorts of statements - some crossing the line into rumours and innuendo - about what the study does and does not mean.
What the study disproves
As mentioned above, science is largely about disproving something. In this case anyone who's been part of this conversation should understand that the study is about disproving the lipid-heart hypothesis. One version of that hypothesis is as follows:
“Lifetime exposure to high levels of ApoB containing lipoprotein (the most famous of which is LDL) is causally associated with the buildup of plaque in the coronary arteries in a dose dependent way and through this mechanism cause heart disease including heart attacks.”
That's a complicated way of saying that ApoB/LDL causes heart disease and lower ApoB/LDL is always better for those who want to minimise their chance of getting a heart attack. That hypothesis is very much accepted by the mainstream literature. If you doubt that, you can read this paper or this one or many many more.
This study looked at 100 people who were otherwise healthy with sky high ApoB (and LDL) and also with low triglycerides and high HDL. Given the lipid heart hypothesis, one would have expected those with higher ApoB to see higher plaque progression. And that’s simply not what the data shows.
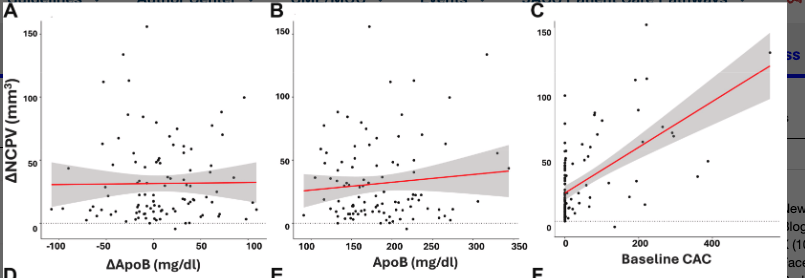
These three charts are looking at the change in non-calcified plaque volume (NCPV) and seeing if that correlates with either ApoB, change in ApoB or baseline calcified plaque (CAC). And of those three there is only a correlation between baseline CAC and plaque progression. Hence the title of the paper “plaque begets plaque”. (I happen to think that this correlation isn’t strong enough to draw conclusions, as I’ll explain below.)
If your hypothesis is that high ApoB is always associated with greater plaque progression, this data set is enough to disprove it.
What it doesn’t prove
So far I haven’t found anyone online arguing against what I’ve written above. Instead, critics are complaining that the study doesn’t prove what they think it should prove.
Let’s address some of the criticisms:
But the LMHR were not protected (they did have some plaque):
That is absolutely true. Why did you think that it wouldn’t be true? Diet is not the only thing that we’re concerned about when we talk about heart disease. This team was not testing the hypothesis “Low carb diets are protective in all cases against heart disease.” Such a hypothesis would be pretty easy to disprove.
The average plaque progression is greater than we see in other cohorts:
Here we have to get into the methodology. This paper uses “high-resolution coronary computed tomography angiography (CCTA) with artificial intelligence-guided plaque quantification” to determine plaque volume. As far as I know it is one of the first papers to use this kind of data. Comparing this data that is gathered using AI with supposedly similar data that doesn’t use AI may not be an “apples to apples” comparison. If there is data using the same methodology showing that the disease progression is on average higher in this cohort, that would be worth exploring. So far I haven't seen it.
All the participants had high ApoB so therefore it doesn’t show anything:
The lipid heart hypothesis predicts that ApoB is causally associated with plaque progression in a dose dependent way. The difference between an LDL of 200 and an LDL of 400 is significant enough that one would expect to see an association between higher numbers and more plaque. And we just don’t see this association. If you want to put forward some other hypothesis, that there is a cutoff of ApoB beyond which it becomes problematic or something, you’re welcome to do so. But the fact that some of the participants with the highest LDL/ApoB also had some of the lowest plaque scores means that such a hypothesis may already be disproven with this data (and lots of similar data sets).
OMG I have a non-zero CAC. Should I panic?
My one criticism with this data and the way this data has been presented is that it lends itself to this conclusion. But if you dive a little deeper you’ll find that the correlation between pre-existing plaque and disease progression is still pretty weak.
As a reminder, whenever we have this kind of a data set we are always looking at association. Associations can never prove causation, but if the association is 100% (an R squared of 1.0) that’s a pretty good indicator that one is causing the other. For example there is always an association between the incidence of lightning and the incidence of thunder, so we know that one is causing the other. That’s an extreme example, but most statisticians will tell you that an R squared of 0.7 (70%) or more is a good indication that we’re seeing what could be a causal relationship.
So what’s the R squared here? 0.33, meaning that disease progression was correlated with existing plaque scores roughly 1 out of 3 times. That’s way better than the R squared for ApoB which was -0.01, but still not enough to indicate causation. If I had a non-zero plaque score, these data wouldn't concern me more than I would have already been. I would just keep monitoring disease progression, through annual CAC scans and getting worried if the CAC progression was at more than 10% annually.
So what is really going on here?
The short answer is we don’t know. This study was designed to test a very specific hypothesis. These other questions are largely beyond the scope of what it can address.
But I think there are a couple of case studies from which we can posit a pretty good guess as to what might be going on. The first one that comes to mind is that of Dr. Stephen Hussey, who had a heart attack after he had already been on a low carb diet for some time. He was able to reverse disease progression not by changing his diet (if anything he became more strict after his heart attack) but by focussing on things like sauna, exercise, and red light therapy.
The theoretical framework within which Dr. Hussey is working dates back thousands of years. One point of origin for that framework is Traditional Chinese Medicine (TCM) which has a focus on the idea of blood flow as a basic indicator of health. What determines blood flow? Diet is part of it, but diet is far from the only thing. What about sun exposure? Nitric oxide production? The hormetic effects of heat and cold exposure? Vitamin D? Clotting factors? Blood viscosity?
I have no idea the extent to which any of these are causal in the process of cardiovascular disease in general and plaque formation in particular. But I do know that the myopic focus on LDL/ApoB has been misguided.
"Science progresses one funeral at a time," Max Planck famously observed. This study won’t change cardiology overnight—but it lights a fuse under decades of unquestioned dogma.
The real lesson? Biological systems defy simplicity. Just as emus disprove "all birds fly," lean mass hyper-responders disprove "all high LDL is dangerous." The next frontier isn’t debating LDL—it’s figuring out exactly what is going on here. Unresolved questions include the following:
- Is inflammation the true driver? If so, what's causing the inflammation?
- Do microvascular dynamics matter more than cholesterol? If so, what's causing the microvascular damage?
- Could plaque be a response to injury, not just a cause? If so, is there something in the immune response that makes some people more prone to heart disease than others?
The best science doesn’t confirm our biases—it shatters them. This study does exactly that. And it also, by virtue of the questions it doesn't answer, indicates the way forward in terms of the research agenda for the next decade or two.
🌱 Ready to Find Your Path to Gut Freedom?
Stop trying to solve your Crohn's, Colitis, or IBD alone with conflicting advice. A personalized plan is the fastest way to clarity and relief.
On a free call, you’ll get:
✅ Clarity on your triggers – Identify the dietary and lifestyle factors uniquely impacting you.
✅ A tailored starting point – Get actionable steps to reduce inflammation and calm your gut.
✅ Real answers – Ask anything about your symptoms and healing (no topic is off-limits).
💬 “Working with Sameer gave me a clear path when I felt completely lost. This is the guidance I needed.” – Previous Client
Your personalized plan is a conversation away.
